Understanding Hormone Testing: Why saliva might be the best choice
As women transition through perimenopause and into postmenopause, many experience changes in hormone levels that can affect their energy, mood, sleep, weight, and overall well-being. Hormone Replacement Therapy (HRT) is often used to help manage these symptoms and restore balance. But how do we know if your treatment is working?
That’s where hormone testing comes in
Traditionally, blood (serum) tests have been the standard method for measuring hormone levels. However, advances in medical testing have introduced a powerful alternative: saliva hormone testing. This method offers a more accurate and personalized way to evaluate hormone levels—especially for women using HRT.
Let’s explore why saliva testing may be a better option for many women in this stage of life.
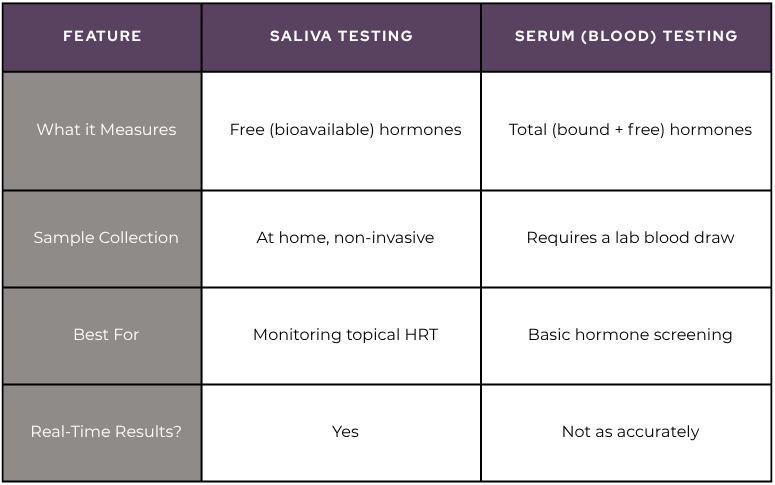
Saliva vs. Serum Testing: What’s the difference?
Why Saliva testing works better for HRT
Topical or sublingual HRT absorbs directly into tissues—not your bloodstream. This means blood tests may not reflect what’s available to your cells.
Saliva testing measures the active, free hormones in your tissues, giving you and your provider a clearer picture.
Especially helpful for
Estradiol
Progesterone
Testosterone
Cortisol (stress hormone)
Advantages of Saliva Testing
Convenient & Stress-Free: Collect at home—no needles, no clinic visits.
Ideal for Topical HRT: Reflects hormone levels that reach your tissues.
More Personalized: Captures daily fluctuations for better dosing accuracy.
Cost-Effective & Non-Invasive: No lab fees or blood draws. Just a simple saliva sample.
Who Should Consider Saliva Testing?
Women in perimenopause (irregular periods, mood swings, hot flashes)
Postmenopausal women on HRT
Anyone seeking a personalized look at hormone balance
Final Thoughts
Hormone balance is not one-size-fits-all.
Saliva testing offers a deeper, more accurate view of your hormones—helping you fine-tune treatment and feel like yourself again.
To schedule an appointment with one of our certified Functional Medicine Physicians, please give us a call. We are excited to partner with you on your journey to optimize your health and wellness through personalized care tailored to your unique needs.
The hormonal shifts that accompany perimenopause and menopause lack a clear instruction manual, often leaving many women in a continuous cycle of trial and error when it comes to managing their symptoms. Fortunately, one of the most potent tools available for regaining control of your hormones is the food you consume. Certain foods contribute to hormone balance and can help alleviate perimenopause and menopause symptoms, while others can disrupt your body’s hormonal equilibrium.
When essential nutritional elements are lacking, hormonal imbalances can arise, leading to mood swings, weight gain, hot flashes, and reduced libido. The primary hormones affected during perimenopause and menopause are estrogen, progesterone, insulin, and testosterone, and your dietary choices can significantly impact these hormones. For instance, excessive sugar consumption can elevate insulin levels, trigger inflammation, and exacerbate nearly every perimenopausal symptom. On the other hand, incorporating vegetables, fruits, nuts, and seeds into your diet can provide phytonutrients and healthy fats that aid in managing even the most challenging menopause symptoms.
While there’s no one-size-fits-all diet, several foods have proven beneficial for most people seeking to balance their hormones:
1. Brassica (aka cruciferous) Vegetables: These include broccoli, cauliflower, kale, and cabbage, which contain indole-3-carbinol—a compound that helps metabolize estrogen in the gut and liver. This can be particularly helpful in addressing estrogen dominance.
2. Healthy Fats: Avocados, nuts, seeds, and fish are rich inomega-3 fatty acids and other fats crucial for reducing inflammation and supporting hormone production, especially progesterone.
3. Fiber-Rich Foods: Fiber is essential for gut health, which plays a critical role in hormone balance. Low-starch fruits and veggies, nuts, seeds, and whole grains can boost your fiber intake, aiding in estrogen metabolism and blood sugar regulation.
However, there are also foods and drinks that should be limited or avoided:
1. Caffeine: Excess caffeine can lead to increased stress hormone production and elevated cortisol levels, potentially exacerbating fatigue and estrogen levels.
2. Processed Carbs and Sugar: As tolerance to sugar decreases with age, limiting simple carbohydrates and sugars (like table sugar, baked goods, and packaged foods) becomes crucial for managing blood sugar and insulin levels.
3. Alcohol: Even moderate alcohol consumption can disrupt hormones, affect brain aging, and lead to elevated insulin levels and estrogen dominance.
4. Gluten: Gluten sensitivity can contribute to gut issues, thyroid problems, and autoimmune conditions, making it advisable to assess its impact on your health
Balancing your diet can ease the transition into perimenopause and menopause, regardless of whether you’re just beginning to experience symptoms or are already in the midst of them. By making thoughtful dietary choices, you can navigate this phase of life with greater vitality and well-being.
Osteoporosis refers to a condition where bones become brittle. A report from the Surgeon General states in the US 54 million Americans are at risk for osteoporosis, and 10 million Americans already have osteoporosis. Although women make up 80% of osteoporosis cases, men still get osteoporosis. Each year 1.5 million people suffer a fracture from bone loss, and if this is a hip fracture, mortality in the first year can be as high as 40%, with higher mortality rates in men than in women. Starting in childhood, there is a fine balance between the building up and breaking down of bones coordinated beautifully between cells named osteoblasts and osteoclasts, respectively. If there is too much osteoclast activity, then there is an increased amount of breakdown of bone as seen in inflammation. There is also this misconception that it is the lack of calcium causing osteoporosis. It is actually calcium balance and not the total calcium which is important in osteoporosis.
Risk factors for osteoporosis include: 1) Aging: Inflammation is a normal process of aging, which increases with age, in functional medicine, this is termed “inflamm-aging”. 2) Diet- SAD: Diet (Standard American Diet) is very inflammatory, upregulating the immune system. Consumption of excess amounts of sugar, alcohol, caffeine, salt, and soda all can lead to bone loss due to demineralization of the bones. A leaky gut can drive inflammation to the point of bone resorption. 3) Lifestyle: Stress, smoking, inactive lifestyle can all contribute to an increased rate of breakdown of bone compared to a build-up of bone. 4) Genes: For instance, Celiac disease predisposes to osteoporosis due to poor absorption of minerals. 5) Gender: Being a female increases the risk, since it is usually seen after menopause because estrogen is protective for the bones as well as the brain and the heart. During menopause estrogen declines and there is no further protection for the bones. 6) Medications: Steroids, proton pump inhibitors (omeprazole, pantoprazole, esomeprazole), cancer drugs, thyroid hormone, cyclosporine, heparin, and warfarin.
Testing for osteoporosis is done thru a DEXA scan. It is also known as a Dual Energy X-ray Absorptiometry, or Bone Density scan, a simple X-ray where the hip and the spine bone density are measured. T-score represents the difference in your bone density from the average bone density of healthy young adults. If the T-score is -1 to -2.5 it is considered osteopenia, if <-2.5 osteoporosis. Osteopenia refers to the beginning of osteoporosis, meaning “bone poverty”.
Treatment of osteoporosis by conventional medicine involves using strong drugs, sometimes too strong which may even cause a break in the bones.
1. Bisphosphonates: i.e., Fosamax, Boniva, Actonel, and Reclast target areas of high turnover where the osteoclasts, cells which break down old bone, absorb bisphosphonate and hence their activity is slowed down and there is a reduction in bone breakdown. Side effects: bone, joint, muscle pain, nausea, gastric ulcer, stress fracture of the thigh bone
2. SERM: Selective estrogen receptor modulator- i.e.Raloxifene, acts like estrogen in some parts of the body but blocks the effects of estrogen in other parts. Increases bone density and reduces the risk of spine fractures, but it has not been shown to decrease the risk of non-spinal fractures. Raloxifene also decreases the risk of invasive breast cancer. Side effects: hot flashes, leg cramps, or blood clots in the legs or lungs. Raloxifene is not recommended for premenopausal women.
3. Parathyroid hormone molecule: i.e. Teriparatide, abaloparatide stimulates new bone formation, rather than preventing bone breakdown. Because of potential safety concerns, particularly an increased risk of bone cancer in rats, the use of this drug is restricted to men and women with severe osteoporosis—who have a high risk of a fracture—and can be given for no more than two years. Side effects: uncommon but may include leg cramps, headaches, dizziness, high blood calcium, and high urinary calcium (with an increased risk of kidney stones). This medication is not recommended for premenopausal women.
4. Romosuzumab: Bone-building medication that is given once a month as pair of injections by a doctor or nurse. Treatment is given once a month for twelve months and is then followed by another medication to prevent bone loss. Romosozumab reduces the risk of spine fractures and non-spine fractures, including hip fractures. Romosozumab may increase the risk of heart attack or stroke—including fatal heart attack or stroke—and it should not be given to women who have had a heart attack or stroke in the past year. It is approved for the treatment of osteoporosis in women past the time of menopause who are at high risk for fracture, defined as a history of osteoporotic fracture, multiple risk factors for fracture, or failure or intolerance to other available osteoporosis therapies. It may cause side effects such as headaches or joint pain.
5. Estrogen hormone therapy: Prevents bone loss and reduces the risk of fracture in the spine and hip. It can also relieve other symptoms of menopause, such as hot flashes and vaginal dryness. Estrogen is usually given in pill form, although it is also available in other forms such as a skin patch or gel. Studies show that the risks of oral estrogen therapy—including heart attack, stroke, blood clots, and breast cancer—may outweigh its benefits in many older women, depending upon the dose and specific preparation. For this reason, estrogen therapy is not usually prescribed solely for fracture prevention.
A comprehensive functional medicine approach to the evaluation of osteoporosis takes the form of blood, saliva, stool, and urine testing. Low-grade inflammation can be assessed thru blood work by checking hs-CRP, HgA1C, ESR, CMP, CBC, and essential fatty acids. Blood work for vitamin D and osteocalcin is necessary since vitamin D helps absorb calcium into the bones and osteocalcin is a biomarker for functional vitamin K deficiency. Bone resorption can be evaluated by urine N-telopeptide. Stool analysis to evaluate the gut is also important since calprotectin in stool provides information about inflammation in the gut. Gut microbes are responsible for making vitamin K, which is necessary for having better bone density. Saliva testing for hormones would provide information about the levels of estradiol, testosterone, DHEA, cortisol, and progesterone.
A comprehensive functional medicine approach to the treatment of osteoporosis is first and foremost prevention. It is recommended by conventional doctors to get a DEXA scan once a woman turns 65, however, it may be too late for some since many risk factors play a role in developing osteoporosis. It is ideal to have a DEXA scan around ages 30-35 as a baseline since this is the time of peak bone mass, and then another one a year after menopause to compare the degree of bone loss to get ahead of the condition.
Osteoporosis refers to a condition where bones become brittle. A report from the Surgeon General states in the US 54 million Americans are at risk for osteoporosis, and 10 million Americans already have osteoporosis. Although women make up 80% of osteoporosis cases, men still get osteoporosis. Each year 1.5 million people suffer a fracture from bone loss, and if this is a hip fracture, mortality in the first year can be as high as 40%, with higher mortality rates in men than in women.
Starting in childhood, there is a fine balance between the building up and breaking down of bones coordinated beautifully between cells named osteoblasts and osteoclasts, respectively. If there is too much osteoclast activity, then there is an increased amount of breakdown of bone as seen in inflammation. There is also this misconception that it is the lack of calcium causing osteoporosis. It is actually calcium balance and not the total calcium which is important in osteoporosis.
Risk factors for osteoporosis include: 1) Aging: Inflammation is a normal process of aging, which increases with age, in functional medicine, this is termed “inflamm-aging”. 2) Diet- SAD: Diet (Standard American Diet) is very inflammatory, upregulating the immune system. Consumption of excess amounts of sugar, alcohol, caffeine, salt, and soda all can lead to bone loss due to demineralization of the bones. A leaky gut can drive inflammation to the point of bone resorption. 3) Lifestyle: Stress, smoking, inactive lifestyle can all contribute to an increased rate of breakdown of bone compared to a build-up of bone. 4) Genes: For instance, Celiac disease predisposes to osteoporosis due to poor absorption of minerals. 5) Gender: Being a female increases the risk, since it is usually seen after menopause because estrogen is protective for the bones as well as the brain and the heart. During menopause estrogen declines and there is no further protection for the bones. 6) Medications: Steroids, proton pump inhibitors (omeprazole, pantoprazole, esomeprazole), cancer drugs, thyroid hormone, cyclosporine, heparin, and warfarin.
Testing for osteoporosis is done thru a DEXA scan. It is also known as a Dual Energy X-ray Absorptiometry, or Bone Density scan, a simple X-ray where the hip and the spine bone density are measured. T-score represents the difference in your bone density from the average bone density of healthy young adults. If the T-score is -1 to -2.5 it is considered osteopenia, if <-2.5 osteoporosis. Osteopenia refers to the beginning of osteoporosis, meaning “bone poverty”.
Treatment of osteoporosis by conventional medicine involves using strong drugs, sometimes too strong which may even cause a break in the bones.
1. Bisphosphonates: i.e., Fosamax, Boniva, Actonel, and Reclast target areas of high turnover where the osteoclasts, cells which break down old bone, absorb bisphosphonate and hence their activity is slowed down and there is a reduction in bone breakdown. Side effects: bone, joint, muscle pain, nausea, gastric ulcer, stress fracture of the thigh bone
2. SERM: Selective estrogen receptor modulator- i.e.Raloxifene, acts like estrogen in some parts of the body but blocks the effects of estrogen in other parts. Increases bone density and reduces the risk of spine fractures, but it has not been shown to decrease the risk of non-spinal fractures. Raloxifene also decreases the risk of invasive breast cancer. Side effects: hot flashes, leg cramps, or blood clots in the legs or lungs. Raloxifene is not recommended for premenopausal women.
3. Parathyroid hormone molecule: i.e. Teriparatide, abaloparatide stimulates new bone formation, rather than preventing bone breakdown. Because of potential safety concerns, particularly an increased risk of bone cancer in rats, the use of this drug is restricted to men and women with severe osteoporosis—who have a high risk of a fracture—and can be given for no more than two years. Side effects: uncommon but may include leg cramps, headaches, dizziness, high blood calcium, and high urinary calcium (with an increased risk of kidney stones). This medication is not recommended for premenopausal women.
4. Romosuzumab: Bone-building medication that is given once a month as pair of injections by a doctor or nurse. Treatment is given once a month for twelve months and is then followed by another medication to prevent bone loss. Romosozumab reduces the risk of spine fractures and non-spine fractures, including hip fractures. Romosozumab may increase the risk of heart attack or stroke—including fatal heart attack or stroke—and it should not be given to women who have had a heart attack or stroke in the past year. It is approved for the treatment of osteoporosis in women past the time of menopause who are at high risk for fracture, defined as a history of osteoporotic fracture, multiple risk factors for fracture, or failure or intolerance to other available osteoporosis therapies. It may cause side effects such as headaches or joint pain.
5. Estrogen hormone therapy: Prevents bone loss and reduces the risk of fracture in the spine and hip. It can also relieve other symptoms of menopause, such as hot flashes and vaginal dryness. Estrogen is usually given in pill form, although it is also available in other forms such as a skin patch or gel. Studies show that the risks of oral estrogen therapy—including heart attack, stroke, blood clots, and breast cancer—may outweigh its benefits in many older women, depending upon the dose and specific preparation. For this reason, estrogen therapy is not usually prescribed solely for fracture prevention.
A comprehensive functional medicine approach to the evaluation of osteoporosis takes the form of blood, saliva, stool, and urine testing. Low-grade inflammation can be assessed thru blood work by checking hs-CRP, HgA1C, ESR, CMP, CBC, and essential fatty acids. Blood work for vitamin D and osteocalcin is necessary since vitamin D helps absorb calcium into the bones and osteocalcin is a biomarker for functional vitamin K deficiency. Bone resorption can be evaluated by urine N-telopeptide. Stool analysis to evaluate the gut is also important since calprotectin in stool provides information about inflammation in the gut. Gut microbes are responsible for making vitamin K, which is necessary for having better bone density. Saliva testing for hormones would provide information about the levels of estradiol, testosterone, DHEA, cortisol, and progesterone.
A comprehensive functional medicine approach to the treatment of osteoporosis is first and foremost prevention. It is recommended by conventional doctors to get a DEXA scan once a woman turns 65, however, it may be too late for some since many risk factors play a role in developing osteoporosis. It is ideal to have a DEXA scan around ages 30-35 as a baseline since this is the time of peak bone mass, and then another one a year after menopause to compare the degree of bone loss to get ahead of the condition.
Once you have osteoporosis then the treatment is as follows:
Exercise: At least 3 days a week, if you don’t use your bones you will lose them. Weightlifting, bands, core strengthening, and yoga all help with building up bone mass and also help preserve balance.
Optimize vitamin D levels: In osteoporosis, you need higher levels of vitamin D, ideally 80-100. This usually amounts to 5000 IU daily and needs to be taken along with vitamin K2 which helps absorb the Calcium into the bones in place of the arteries.
Diet: Eliminate “bone dissolvers”: excess protein, SAD processed diet, excess salt. Obtain Calcium from your diet as much as possible and not supplements. Add more greens to your diet, herring, mackerel, sesame seeds, and chia seeds are all excellent sources of calcium.
Hormones: Low testosterone and low estrogen can cause bone loss, and higher levels of FSH in menopause are associated with higher osteoclast activity. Hormone supplementation may help.
Nutraceuticals: Trace minerals are extremely important in building bone, such as magnesium, zinc, boron, manganese, copper, and silicon. If you are taking Calcium then make sure it’s in a microcrystalline hydroxyapatite complex which provides bone-enhancing factors such as growth factors, peptides, and mucopolysaccharides.