For many Valentine’s Day brings with it thoughts of chocolate. February is both American Heart Month and National Chocolate Lovers Month, a brilliant combination as the nutrients within chocolate can help to improve heart health. Let’s dig into the good, the bad, and the ugly of chocolate.
Dark chocolate is rich in polyphenols, specifically flavonoids, the substances that have a wide range of health benefits. These include lowering blood pressure, improving the function of our vascular endothelium (the inner walls of our arteries), protecting skin against sun damage, improving blood flow to the brain, and reducing the risk of cardiovascular damage. Dark chocolate has also been proven to help with mood. These benefits come from chocolate’s ability to promote production of the vasodilator Nitric Oxide as well as the anandamide within, a cannabinoid compound (like CBD) that binds to receptors in the brain to alter mood and brain activity. In addition, methylxanthine compounds, such as theobromine and caffeine, are powerful antioxidants. Remember that these are stimulants as well and should be kept far from your bedtime.
As milk chocolate has a much higher sugar content and lower flavonoid content, dark chocolate, at least 70%, is the best choice. Know that white chocolate has no flavonoids, and hot chocolate mixes have very low amounts. As even dark chocolate has sugar, limiting daily intake to 1 oz of at least 70% dark chocolate is the best choice.
There is however, a DARK side to chocolate: heavy metals. Lead and cadmium have been known for many years to be elevated in chocolate. Consumer reports has recently reported their results of batch metals testing of multiple brands of chocolate. They have confirmed levels of metals in many brands of chocolate that exceed California Proposition 65 standards, specifically for lead and cadmium. These metals are associated with multiple health issues in both children and adults. The risk is highest for young children and pregnant women as metals have a negative effect on brain development and IQ. However, even outside this patient population, accumulation of metals in the body can cause a wide range of health conditions including kidney damage, elevated blood pressure, immune and hormonal disruption, and central nervous system dysfunction.
Now why would metals be in our chocolate? For cadmium, the cacao plant absorbs the metals from the soil and levels accumulate in the beans. Lead, however, gets in after harvesting, with levels rising as the beans dry and are processed. Highest levels are found on the outside of the bean, consistent with environmental contamination.
So…. should we give up chocolate? My vote is a resounding NO! The “Yum” and “Aaaaah” response to chocolate are undeniable, and the health benefits are substantial and backed by science. The Consumer Reports study gives us guidance as to which brands of dark chocolate are lowest in metals. See the report for details where one bar each from Mast, Tatza, and Valrhona, and two bars from Ghirardelli have relative low levels of both cadmium and lead
From the Functional Medicine perspective, food is medicine. But the devil is in the details where purity, dose and timing make it medicine or poison. Choose your brand wisely, be moderate in your amount, and time your chocolate well away from your bedtime. And most of all: ENJOY!
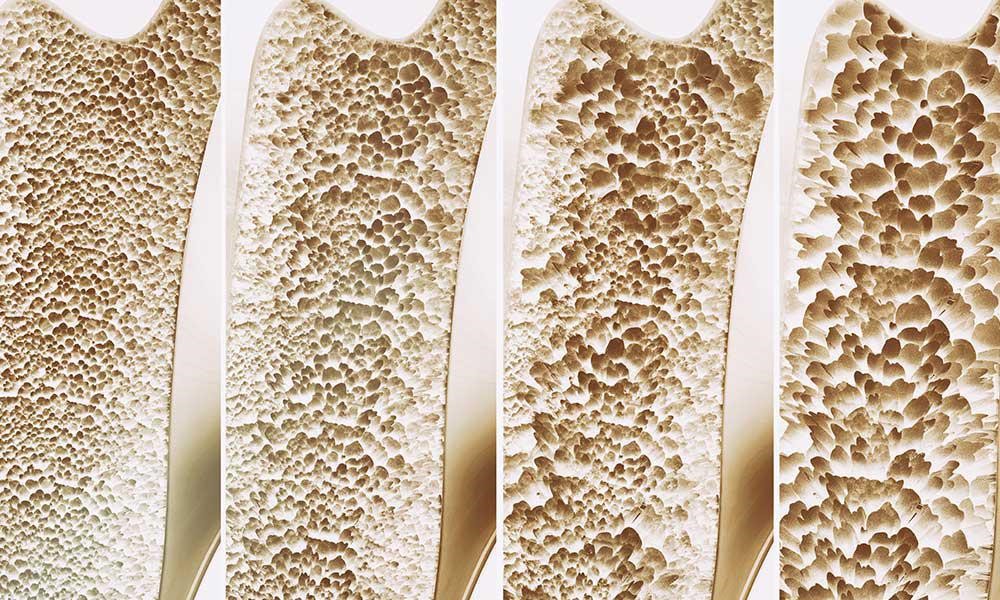
Osteoporosis refers to a condition where bones become brittle. A report from the Surgeon General states in the US 54 million Americans are at risk for osteoporosis, and 10 million Americans already have osteoporosis. Although women make up 80% of osteoporosis cases, men still get osteoporosis. Each year 1.5 million people suffer a fracture from bone loss, and if this is a hip fracture, mortality in the first year can be as high as 40%, with higher mortality rates in men than in women. Starting in childhood, there is a fine balance between the building up and breaking down of bones coordinated beautifully between cells named osteoblasts and osteoclasts, respectively. If there is too much osteoclast activity, then there is an increased amount of breakdown of bone as seen in inflammation. There is also this misconception that it is the lack of calcium causing osteoporosis. It is actually calcium balance and not the total calcium which is important in osteoporosis.
Risk factors for osteoporosis include: 1) Aging: Inflammation is a normal process of aging, which increases with age, in functional medicine, this is termed “inflamm-aging”. 2) Diet- SAD: Diet (Standard American Diet) is very inflammatory, upregulating the immune system. Consumption of excess amounts of sugar, alcohol, caffeine, salt, and soda all can lead to bone loss due to demineralization of the bones. A leaky gut can drive inflammation to the point of bone resorption. 3) Lifestyle: Stress, smoking, inactive lifestyle can all contribute to an increased rate of breakdown of bone compared to a build-up of bone. 4) Genes: For instance, Celiac disease predisposes to osteoporosis due to poor absorption of minerals. 5) Gender: Being a female increases the risk, since it is usually seen after menopause because estrogen is protective for the bones as well as the brain and the heart. During menopause estrogen declines and there is no further protection for the bones. 6) Medications: Steroids, proton pump inhibitors (omeprazole, pantoprazole, esomeprazole), cancer drugs, thyroid hormone, cyclosporine, heparin, and warfarin.
Testing for osteoporosis is done thru a DEXA scan. It is also known as a Dual Energy X-ray Absorptiometry, or Bone Density scan, a simple X-ray where the hip and the spine bone density are measured. T-score represents the difference in your bone density from the average bone density of healthy young adults. If the T-score is -1 to -2.5 it is considered osteopenia, if <-2.5 osteoporosis. Osteopenia refers to the beginning of osteoporosis, meaning “bone poverty”.
Treatment of osteoporosis by conventional medicine involves using strong drugs, sometimes too strong which may even cause a break in the bones.
1. Bisphosphonates: i.e., Fosamax, Boniva, Actonel, and Reclast target areas of high turnover where the osteoclasts, cells which break down old bone, absorb bisphosphonate and hence their activity is slowed down and there is a reduction in bone breakdown. Side effects: bone, joint, muscle pain, nausea, gastric ulcer, stress fracture of the thigh bone
2. SERM: Selective estrogen receptor modulator- i.e.Raloxifene, acts like estrogen in some parts of the body but blocks the effects of estrogen in other parts. Increases bone density and reduces the risk of spine fractures, but it has not been shown to decrease the risk of non-spinal fractures. Raloxifene also decreases the risk of invasive breast cancer. Side effects: hot flashes, leg cramps, or blood clots in the legs or lungs. Raloxifene is not recommended for premenopausal women.
3. Parathyroid hormone molecule: i.e. Teriparatide, abaloparatide stimulates new bone formation, rather than preventing bone breakdown. Because of potential safety concerns, particularly an increased risk of bone cancer in rats, the use of this drug is restricted to men and women with severe osteoporosis—who have a high risk of a fracture—and can be given for no more than two years. Side effects: uncommon but may include leg cramps, headaches, dizziness, high blood calcium, and high urinary calcium (with an increased risk of kidney stones). This medication is not recommended for premenopausal women.
4. Romosuzumab: Bone-building medication that is given once a month as pair of injections by a doctor or nurse. Treatment is given once a month for twelve months and is then followed by another medication to prevent bone loss. Romosozumab reduces the risk of spine fractures and non-spine fractures, including hip fractures. Romosozumab may increase the risk of heart attack or stroke—including fatal heart attack or stroke—and it should not be given to women who have had a heart attack or stroke in the past year. It is approved for the treatment of osteoporosis in women past the time of menopause who are at high risk for fracture, defined as a history of osteoporotic fracture, multiple risk factors for fracture, or failure or intolerance to other available osteoporosis therapies. It may cause side effects such as headaches or joint pain.
5. Estrogen hormone therapy: Prevents bone loss and reduces the risk of fracture in the spine and hip. It can also relieve other symptoms of menopause, such as hot flashes and vaginal dryness. Estrogen is usually given in pill form, although it is also available in other forms such as a skin patch or gel. Studies show that the risks of oral estrogen therapy—including heart attack, stroke, blood clots, and breast cancer—may outweigh its benefits in many older women, depending upon the dose and specific preparation. For this reason, estrogen therapy is not usually prescribed solely for fracture prevention.
A comprehensive functional medicine approach to the evaluation of osteoporosis takes the form of blood, saliva, stool, and urine testing. Low-grade inflammation can be assessed thru blood work by checking hs-CRP, HgA1C, ESR, CMP, CBC, and essential fatty acids. Blood work for vitamin D and osteocalcin is necessary since vitamin D helps absorb calcium into the bones and osteocalcin is a biomarker for functional vitamin K deficiency. Bone resorption can be evaluated by urine N-telopeptide. Stool analysis to evaluate the gut is also important since calprotectin in stool provides information about inflammation in the gut. Gut microbes are responsible for making vitamin K, which is necessary for having better bone density. Saliva testing for hormones would provide information about the levels of estradiol, testosterone, DHEA, cortisol, and progesterone.
A comprehensive functional medicine approach to the treatment of osteoporosis is first and foremost prevention. It is recommended by conventional doctors to get a DEXA scan once a woman turns 65, however, it may be too late for some since many risk factors play a role in developing osteoporosis. It is ideal to have a DEXA scan around ages 30-35 as a baseline since this is the time of peak bone mass, and then another one a year after menopause to compare the degree of bone loss to get ahead of the condition.
Osteoporosis refers to a condition where bones become brittle. A report from the Surgeon General states in the US 54 million Americans are at risk for osteoporosis, and 10 million Americans already have osteoporosis. Although women make up 80% of osteoporosis cases, men still get osteoporosis. Each year 1.5 million people suffer a fracture from bone loss, and if this is a hip fracture, mortality in the first year can be as high as 40%, with higher mortality rates in men than in women.
Starting in childhood, there is a fine balance between the building up and breaking down of bones coordinated beautifully between cells named osteoblasts and osteoclasts, respectively. If there is too much osteoclast activity, then there is an increased amount of breakdown of bone as seen in inflammation. There is also this misconception that it is the lack of calcium causing osteoporosis. It is actually calcium balance and not the total calcium which is important in osteoporosis.
Risk factors for osteoporosis include: 1) Aging: Inflammation is a normal process of aging, which increases with age, in functional medicine, this is termed “inflamm-aging”. 2) Diet- SAD: Diet (Standard American Diet) is very inflammatory, upregulating the immune system. Consumption of excess amounts of sugar, alcohol, caffeine, salt, and soda all can lead to bone loss due to demineralization of the bones. A leaky gut can drive inflammation to the point of bone resorption. 3) Lifestyle: Stress, smoking, inactive lifestyle can all contribute to an increased rate of breakdown of bone compared to a build-up of bone. 4) Genes: For instance, Celiac disease predisposes to osteoporosis due to poor absorption of minerals. 5) Gender: Being a female increases the risk, since it is usually seen after menopause because estrogen is protective for the bones as well as the brain and the heart. During menopause estrogen declines and there is no further protection for the bones. 6) Medications: Steroids, proton pump inhibitors (omeprazole, pantoprazole, esomeprazole), cancer drugs, thyroid hormone, cyclosporine, heparin, and warfarin.
Testing for osteoporosis is done thru a DEXA scan. It is also known as a Dual Energy X-ray Absorptiometry, or Bone Density scan, a simple X-ray where the hip and the spine bone density are measured. T-score represents the difference in your bone density from the average bone density of healthy young adults. If the T-score is -1 to -2.5 it is considered osteopenia, if <-2.5 osteoporosis. Osteopenia refers to the beginning of osteoporosis, meaning “bone poverty”.
Treatment of osteoporosis by conventional medicine involves using strong drugs, sometimes too strong which may even cause a break in the bones.
1. Bisphosphonates: i.e., Fosamax, Boniva, Actonel, and Reclast target areas of high turnover where the osteoclasts, cells which break down old bone, absorb bisphosphonate and hence their activity is slowed down and there is a reduction in bone breakdown. Side effects: bone, joint, muscle pain, nausea, gastric ulcer, stress fracture of the thigh bone
2. SERM: Selective estrogen receptor modulator- i.e.Raloxifene, acts like estrogen in some parts of the body but blocks the effects of estrogen in other parts. Increases bone density and reduces the risk of spine fractures, but it has not been shown to decrease the risk of non-spinal fractures. Raloxifene also decreases the risk of invasive breast cancer. Side effects: hot flashes, leg cramps, or blood clots in the legs or lungs. Raloxifene is not recommended for premenopausal women.
3. Parathyroid hormone molecule: i.e. Teriparatide, abaloparatide stimulates new bone formation, rather than preventing bone breakdown. Because of potential safety concerns, particularly an increased risk of bone cancer in rats, the use of this drug is restricted to men and women with severe osteoporosis—who have a high risk of a fracture—and can be given for no more than two years. Side effects: uncommon but may include leg cramps, headaches, dizziness, high blood calcium, and high urinary calcium (with an increased risk of kidney stones). This medication is not recommended for premenopausal women.
4. Romosuzumab: Bone-building medication that is given once a month as pair of injections by a doctor or nurse. Treatment is given once a month for twelve months and is then followed by another medication to prevent bone loss. Romosozumab reduces the risk of spine fractures and non-spine fractures, including hip fractures. Romosozumab may increase the risk of heart attack or stroke—including fatal heart attack or stroke—and it should not be given to women who have had a heart attack or stroke in the past year. It is approved for the treatment of osteoporosis in women past the time of menopause who are at high risk for fracture, defined as a history of osteoporotic fracture, multiple risk factors for fracture, or failure or intolerance to other available osteoporosis therapies. It may cause side effects such as headaches or joint pain.
5. Estrogen hormone therapy: Prevents bone loss and reduces the risk of fracture in the spine and hip. It can also relieve other symptoms of menopause, such as hot flashes and vaginal dryness. Estrogen is usually given in pill form, although it is also available in other forms such as a skin patch or gel. Studies show that the risks of oral estrogen therapy—including heart attack, stroke, blood clots, and breast cancer—may outweigh its benefits in many older women, depending upon the dose and specific preparation. For this reason, estrogen therapy is not usually prescribed solely for fracture prevention.
A comprehensive functional medicine approach to the evaluation of osteoporosis takes the form of blood, saliva, stool, and urine testing. Low-grade inflammation can be assessed thru blood work by checking hs-CRP, HgA1C, ESR, CMP, CBC, and essential fatty acids. Blood work for vitamin D and osteocalcin is necessary since vitamin D helps absorb calcium into the bones and osteocalcin is a biomarker for functional vitamin K deficiency. Bone resorption can be evaluated by urine N-telopeptide. Stool analysis to evaluate the gut is also important since calprotectin in stool provides information about inflammation in the gut. Gut microbes are responsible for making vitamin K, which is necessary for having better bone density. Saliva testing for hormones would provide information about the levels of estradiol, testosterone, DHEA, cortisol, and progesterone.
A comprehensive functional medicine approach to the treatment of osteoporosis is first and foremost prevention. It is recommended by conventional doctors to get a DEXA scan once a woman turns 65, however, it may be too late for some since many risk factors play a role in developing osteoporosis. It is ideal to have a DEXA scan around ages 30-35 as a baseline since this is the time of peak bone mass, and then another one a year after menopause to compare the degree of bone loss to get ahead of the condition.
Once you have osteoporosis then the treatment is as follows:
Exercise: At least 3 days a week, if you don’t use your bones you will lose them. Weightlifting, bands, core strengthening, and yoga all help with building up bone mass and also help preserve balance.
Optimize vitamin D levels: In osteoporosis, you need higher levels of vitamin D, ideally 80-100. This usually amounts to 5000 IU daily and needs to be taken along with vitamin K2 which helps absorb the Calcium into the bones in place of the arteries.
Diet: Eliminate “bone dissolvers”: excess protein, SAD processed diet, excess salt. Obtain Calcium from your diet as much as possible and not supplements. Add more greens to your diet, herring, mackerel, sesame seeds, and chia seeds are all excellent sources of calcium.
Hormones: Low testosterone and low estrogen can cause bone loss, and higher levels of FSH in menopause are associated with higher osteoclast activity. Hormone supplementation may help.
Nutraceuticals: Trace minerals are extremely important in building bone, such as magnesium, zinc, boron, manganese, copper, and silicon. If you are taking Calcium then make sure it’s in a microcrystalline hydroxyapatite complex which provides bone-enhancing factors such as growth factors, peptides, and mucopolysaccharides.